
$225.
That is the cost to be a member of ASHA.
But you already know that. You pay that bill every year.
But you might not know there is a “certified nonmember” option.
You can have your CCC, not be an ASHA member, and save $26.
In person and on social media, I’ve seen more and more practitioners discussing this option, saving the money, and ditching ASHA.
If I’m being honest, I’ve thought about it too. But before making that decision, I did some digging.
I read some ASHA membership reports. I reached out to SLPs through social media and in real life. I looked at comparable organizations. And I spoke with Kate Stephens, ASHA’s Senior Director of Membership.
I found out some surprising things, and it really helped me solidify my decision about membership.
Before I tell you which way I’m going, let me tell you what I learned:
- A (brief) history of the “certificate holder only” option
- What it is & how to become one
- Why people are becoming non-members
- The Boycott Club
- Convention Attendee to Boycott
- Diversity, Equity, and Inclusion
- Fact-Checking
- Not-worth-It for me crowd
- The Boycott Club
- How many non-members are there?
- ASHA’s response
The Brief History of the ‘certificate holder only’ Option
Long-story short: ASHA was founded in 1925 under a different name. (Side note: if anyone knows of a good place to learn more about the history of ASHA and our field, let me know please!).
From then until 1978, if you wanted to hold a Certificate of Clinical Competence (in SLP or AuD), you had to be a member of the association.
In 1978 that changed… but not because ASHA wanted it to.
As best as I can understand (because I don’t speak legalese) Dale Bogus, an SLP, sued ASHA arguing that forcing ASHA membership as a requirement for having a CCC was an “unlawful tying arrangement” in violation of the Sherman Act.
Again, I’m not a lawyer. But based on my googling and wikipedia reading, the Sherman Act is a trade law from the 1890’s. It does a lot of things, and one of the biggest things it does is make it illegal to monopolize or (attempt to monopolize) any part of trade or commerce.
Bogus won.
As a result, ASHA created and has continued to offer the “certificate holder only” option to obtain and maintain one’s professional credential without being a member of the association.
For clarity, I’ve seen ASHA call it different things in different places in their publications and website including:
- certificate holder only
- certified nonmembers
- nonmember certificate holders
So, what exactly is a ‘certificate holder-only’?
Straight from ASHA as of the date of publication: “An individual may also choose to apply for certificate-holder status that is, hold the Certificate of Clinical Competence but not become a member of the Association. Non-member certificate holders are not eligible for member benefits.” ~ASHA 2023 Membership Categories
It means you have your Certificate of Clinical Competence (CCC) but are not a member of ASHA.
It is kind of like if ASHA had two jobs (it has a lot more functions in reality, but let’s pretend).
- Job 1: Decide who is qualified to have a CCC and manage that process
- Job 2: Be a club for people who are interested in communication and swallowing stuff
The CCC costs $199 and being a member of the club is another $26.
$199 +$26 = $225
I always assumed you have to be “in the club” in order to have your CCC. But it turns out you don’t.
How do you become a ‘certificate holder-only’?
How do you apply for this status?
ASHA doesn’t make it as easy as paying your dues.
When you want to renew, you have to email, chat with an agent, or call. Basically, you can’t use any of the self-service options. And you’ll have to ask specifically to become a certificate holder only. Note, ASHA’s Director of Membership did share (more below) that the chat function is taken offline intentionally during “peak season” and customer service is funneled to phone and email.
Why some people are becoming non-members
Just because you can do something doesn’t mean you should. So before dropping my ASHA membership, I’ve spent a little time learning more about the issue. It is pretty tempting right, to save the cash.
I found essentially two groups of people that aren’t joining ASHA but are renewing their CCC.
- Those who are boycotting ASHA, and
- Those who don’t see the value in membership
I was surprised to learn a few things talking to people from each camp.
Let’s start with ‘The Boycott Club’
Surprise: it isn’t a club.
I heard a big range of reasons and grievances from across our field and national political spectrum. And it really seems to be reflective of broader culture wars that are playing out across the United States.
Convention Attendee to Boycotter
Jeanne had been hoping for several years to attend an ASHA national convention. She’s been practicing as an SLP since 2011 in the pacific northwest, so she’s had few years to think about it.
2022 was finally going to be the year. Jeanne was planning to attend the convention in New Orleans with a friend from graduate school. Then Roe v. Wade was overturned.
“ASHA said they couldn’t take a stance… I thought that was bullshit. Being silent is being complicit.” Jeanne told me kindly but firmly.
Jeanne and her friend still went to New Orleans, just not to the convention. Well, they didn’t go inside the convention. They posted themselves outside the convention hall and protested. They handed out flyers and talked to passersby about ASHA’s refusal to take a stance on the SCOTUS’s Decision in Dobbs v. Jackson Women’s Health Organization case.
I talked with Jeanne on the phone one morning about her protest of ASHA both at the NOLA convention and beyond. She talked about how ASHA isn’t doing enough, or at least with enough visibility.
So she asked herself, “Why am I paying to maintain my C’s to an organization that thinks bodily autonomy is political?” In response, she plans to renew her C’s as a “certified non-member.” She’ll still have a CCC but she will no longer be a member of ASHA.
Jeanne and I talked at length about the merits of boycotting ASHA by becoming a non-member. When I shared that I’d spoken with other SLPs who are going the non-member route for quite opposite political beliefs, Jeanne responded, “It comes down to personal choice. You can be a certified non-member, and then what are you doing? Tommy and I are doing in a small way the thing we know to do.”
Other SLPs are leaving ASHA because of their policies on diversity, equity, and inclusion
ASHA’s stance on Roe v. Wade (or more specifically the Dobbs vs Jackson Women’s Health Organization that overturned Roe v. Wade) was exactly what Jeanne said it was: ASHA saying it can’t take a stance. You can read the statement here for yourself: https://www.asha.org/about/statements/ASHA-Statement-on-Supreme-Court-Decision-Dobbs-v-Jackson-Womens-Health-Organization/
But ASHA taking a stance (or not) cuts both ways. Some SLPs are leaving ASHA membership behind to protest the fact that ASHA is taking a stance.
Among them is an SLP we’ll call Patty. She asked to remain anonymous because she worries about how quickly the conversation goes from “respectful and rational” to spiteful and vitriolic. So for ease of reading, I’ve made up the name Patty for her.
We dug into why she dropped her membership. And her reasons are parallel to Jeanne’s… but also kind of totally the opposite.
“I am not a member because I do not like the fact that ASHA feels they need to have an opinion, and therefore policy, on social issues,” Patty wrote to me. She went on to refer to some of ASHA’s positions as pandering and virtue signaling.
“How we feel about social issues should not even enter the picture when we step into our roles each morning.”
Patty was a certified member for the first 20 years of her career. She dropped membership for a for few years while living abroad. “When I returned [to the Southwest United States] I reinstated the membership to have access to the research. Then ASHA started with what seemed like a disproportionate amount of focus on equity and gender/sexuality issues. So I dropped it again.”
Changing CEU requirements reflect changing needs and values
The issue of “equity” that Patty mentioned is ASHA’s requirement to obtain, “at least 2 [professional development] hours must be in cultural competency, cultural humility, culturally responsive practice, or diversity, equity, and inclusion (DEI).” https://www.asha.org/certification/prof-dev-for-2020-certification-standards/ It was proposed in 2020 as part of ASHA’s Envisioned Future * https://www.asha.org/about/ashas-envisioned-future/ and is effective as of January 2023.
I asked why Patty was opposed to the requirement. “I feel that this is a construct which is false and a bit of smoke and mirrors because all of us have challenges, setbacks, and disadvantages…I am pretty sure each of us can be trusted to be sensitive and kind without ASHA mandating that we take a CEU on how to be sensitive and kind. I find it insulting that ASHA feels I need to be taught this,” Patty wrote in response.
LGBTQ+ Issues
On issues regarding gender and sexual orientation, Patty shared the example of a recent ASHA leader that, “was totally dedicated to the LBGTQ movement both from providers who are gay and treatment of this population.”
To be clear, Patty did say she thinks it is okay for ASHA to publish about these topics. As long as it isn’t too much, “Just because I’m not personally interested in it, I’m sure others are. If LGBTQ folks are about 5% of the population? Then 5% of the publication space is reasonable?”
Of course, as we discussed LGBTQ+ issues, we discussed voice and communication services for transgender and gender diverse populations. Patty’s position is that gender affirming voice therapies are ultimately vocal abuse.
Fact-Checking Jeanne & Patty:
ASHA Leader dedicated a whole issue to the LGTBQ movement: False.
I asked Patty more about the magazine she referenced, but she couldn’t find her copy. And I don’t blame her – I toss my ASHA Leader pretty quickly too after skimming it.
So, I checked the ASHA Wire (the online home for its journals and publications) (https://pubs.asha.org/) for old Leader, AJA, AJSLP, JSLHR, and LSHSS issues. I couldn’t find any dedicated solely to the topic of the LGBTQ population. The closest I found was the Sept/Oct 2022 issue which mentioned on the cover an article within about “Supporting LGBTQ+ Graduate Students.”
Without a copy of the print version, I can’t say for sure, but reviewing the electronic versions available on the wire shows that just 1 of the 38 articles in that issue included LGBTQ+ issues.
Word-count or square inches of space in the magazine might be the best way to verify Patty’s suggested 5% amount. But 1 article of 38 is about 2.6%.
Gender-Affirming Vocal Therapies are Vocal Abuse: False.
Patty shared she believes gender-affirming vocal therapies are “vocal abuse.” To be clear, my knee-jerk reaction is to disagree with Patty’s statement. But in the interest of fact-checking, I did some searching.
This paper by Sarah Schneider, M.S. CCC-SLP and Mark Courey, MD is a great overview of the topic.
This paper (Working with the transgender voice: The role of the speech and language therapist) by Jane Thornton mentions potentially altered voice quality that is “dysfunctional or unstable” but in the context of the client already having attempted to alter their voice (likely on their own). Thornton writes, “These patterns will be causing vocal abuse and should be eliminated before beginning any gender work.”
Relatedly, there’s surgical interventions to changing the voice. SLPs obviously don’t do the surgery, but I certainly hope they’re involved in pre-surgical and post-surgical processes. Sites I checked out definitely discuss risks of the surgeries (Cleveland Clinic ; Mayo Clinic) . Whether or not benefits outweigh the risks is a very personal decision for an individual to make for themselves, hopefully in consultation with an informed and trusted health care provider. Risk for complications is not the same as abuse.
So, I don’t see any information about these types of interventions being tantamount to vocal abuse, and it certainly doesn’t match my clinical training.
ASHA said they couldn’t take a stance: True.
ASHA literally wrote, “it is beyond the scope of ASHA’s mission and advocacy efforts to take a stand.”
You can and should read ASHA’s full statement on the Dobbs vs Jackson ruling for the complete context. And then compare it to those of other similar organizations.
Here’s a list of comparable organizations and links to their strong statements condemning the SCOTUS Dobbs v. Jackson ruling:
- American Medical Association: https://www.ama-assn.org/about/leadership/dobbs-ruling-assault-reproductive-health-safe-medical-practice
- American Occupation Therapy Association: https://www.aota.org/about/mission-vision/dobbs-v-jackson-womens-health-organization-court-ruling
- American Physical Therapy Association: https://www.apta.org/article/2022/06/27/statement
- American Psychological Association: https://www.apa.org/news/press/releases/2022/06/scotus-abortion-decision
- National Education Associations: https://www.nea.org/about-nea/media-center/press-releases/nea-presidents-statement-dobbs-v-jackson-womens-health-organization
- National Nurses United: https://www.nationalnursesunited.org/press/nurses-condemn-supreme-court-overturn-of-constitutional-right-of-abortion
- American Art Therapy Association: https://arttherapy.org/news-dobbs-v-jackson-statment/
- National Association of Social Workers: https://www.socialworkers.org/News/News-Releases/ID/2505/NASW-Condemns-Decision-by-the-US-Supreme-Court-to-Overturn-Roe-v-Wade
The only related organization I could find without a statement at all was the National Council for Therapeutic Recreation Certification.
Those who don’t see the value in it
Not all SLPs or AuDs who are non-members are doing so for political reasons. The vast majority that I heard from are non-members because they don’t see themselves getting much value from ASHA.
One SLP commented anonymously to me, “and I don’t like to support ASHA because I think they’re out of touch and don’t provide us with the support we deserve (caseload caps, paid on teacher scale, etc). So I pay the minimum.”
Another wrote to me “You can access everything from the Leader online for free, you can email the authors of any research article and 9 times out of 10 they will email it to you for free, tracking your own CEUs only requires 3 seconds to take a picture/screenshot.”
So many SLP’s expressed issues like these that basically amount to not seeing the value in membership.
How many non-member certificate holders are there?
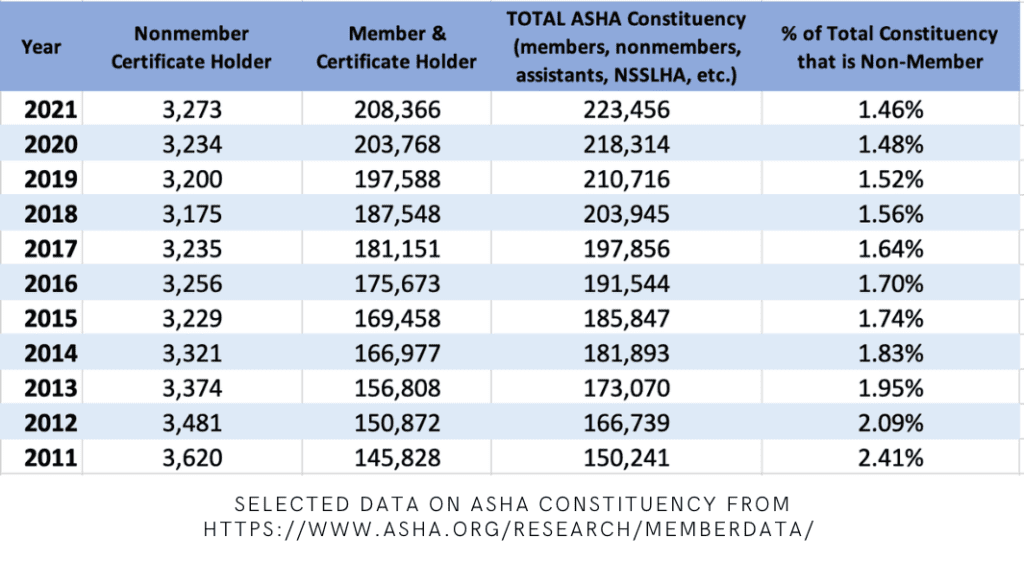
Each year ASHA publishes a “Member and Affiliate Profile” report.
As far as I can see, it goes back to 2011. I went through the reports and pulled out three pieces of information:
- Number of nonmember certificate holders
- Number of members + certificate holders
- Total ASHA constituency (i.e., members, non-members, SLPAs, retired members, etc.)
Here’s the data. Note, the “Total” column, represents total ASHA constituency including members, non-members, and many other affiliation statuses like retired members, honorary ones, etc.
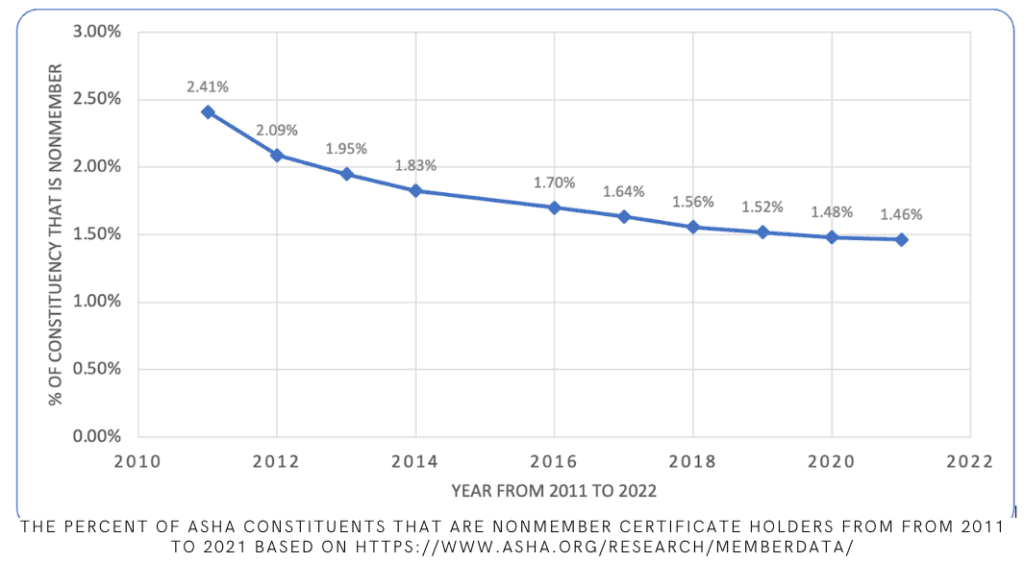
Here is the same data on a scatter plot. As you can see, the overall percentage of nonmembers relative to total constituency has declined significantly. I’m guessing this is due to the growth of overall membership more than a real “decline” in nonmembership.
Thoughts from ASHA’s Senior Director of Membership, Kate Stephens
I contacted the ASHA Board of Directors about this topic.
Would you be surprised to know I got a response? I actually got way more than a response. I got an hour-long conversation with ASHA’s Senior Director of Membership, the professional and personable Kate Stephens.
We started the discussion off about membership and the non-membership option in general. Right off the bat, Kate shared, “this comes at such a great time; we’re actually taking a step back to evalute our member value proposition. We’re thinking about what members want, need, and what we can (and can’t) do for them.”
They are partnering with Long-Dash (a consulting company) to study membership. You might have received an email from them! If you did, I recommend participating. I did, and it was worth it! The results of this study isn’t available yet, but for now, Kate shared how she currently conceptualizes the three types of value in ASHA membership.
- Cost savings for members (e.g. discounts on CEUs, hotels, insurance, etc.)
- Community: access to resources, mentorship programs, Special Interest Groups, etc.
- A Voice in shaping ASHA (i.e., ability to vote on leadership, volunteer on committees, boards, councils, etc.)
I politely told Kate that I think the first area she shared is kind of a fluffy and mostly useless benefit. For example the hotel discounts are often no more than the discounts you find on regular travel websites, and I’ve always been able to obtain better discounts on my insurance in other ways. I’ve never heard of anyone getting much real value out of those available discounts (but if you have, let me know in the comments below!). Kate politely thanked me for the feedback.
As for the “Community value”, we discussed how that is changing as well. For example, I mentioned The Informed SLP and the immense and affordable access it provides to both CEU’s and research. We also briefly discussed how social media is changing community access and connectivity.
Finally, we got to the real heart of it: If you’re a member of ASHA, you get a voice in the association. Kate shared with me in a fair amount of detail about the committees, boards, and councils that in her view “really set the tone for ASHA and the profession more broadly.” And that was something we definitely agreed on. I was surprised to learn that a significant part of ASHA’s work is carried out by SLPs and AuD’s who split their time between clinical practice and working at the national office.
About the Issues
We jumped into the different reasons I’d heard from people about why they’re leaving ASHA, starting with ASHA’s decision not to take a stance on Dobbs v Jackson.
Kate shared, “we have members across the political spectrum. We have members who see abortion (or other issues) as integral to their practice and then members who see the opposite. We are continuing to have very in-depth and personal conversations about where [ASHA’s] lane is, when and how to say things, and when to say something to promote change vs just to say something and add noise.”
In discussing organizations that did and did not take a stance on the SCOTUS ruling, we also discussed the convention, and it being held in a state with draconian laws surrounding reproductive care. Kate is not the mouthpiece for ASHA on these issues (and I didn’t expect her to be), but she was comfortable sharing that ASHA is not the only organization grappling with when and how to respond.
“I recently attended a convention with a session on whether organizations [like ASHA and others] should hold conventions in states with ‘draconian’ laws. Everyone is struggling with this issue,” Kate told me. She added, “It very easily becomes a multifaceted issue. For example, if we don’t have a convention in a certain state, we might be inadvertently limiting access to updated information to professionals in that state or region.”
We ended the discussion about abortion with the idea conversations like this one are going on inside ASHA all the time. “I’m comfortable saying that Vicki Deal-Williams, our CEO, is a very transparent and inclusive leader. She is listening and talking and thinking about these issues constantly,” Kate told me.
I asked Kate about ‘Patty’s’ comments about the “inordinate” focus on LGBTQ issues. And without revealing too much of my personal bias, I was heartened by Kate’s response: “We’re dedicated to supporting our professionals in supporting their patients, and that includes Trans and LGBTQ folks, and that’s not going to change.”
As we wrapped up specifics and broadened our conversation back to membership vs non-membership in general, Kate summarized her position pretty well: “People have a lot of issues with ASHA. Some are legitimate complaints, and some are maybe just misunderstandings about our role. If you have problems with ASHA, come to us. Let’s work through solutions. Get involved. Have the conversation. Understand why things why things are the way they are. That’s where you start if you want to effect change. We want people to be members to have their voices heard and to be engaged. ASHA is its members. They make up the committees, boards, and councils which in turn shape the mission that the professional staff execute and carry out.”
My Decision about my CCC
So you might be wondering what I ended up doing with my CCC and membership.
I ended up renewing the CCC as a member. In the not so distant future, I see myself going the non-member route. But for me, for now, the membership still has value. And right now, being an active member is the best way for me to have my voice heard.
What about you? Are you going to be a non-member? If not, how are you making your voice heard?
Either way, comment below or contact me to share your story!
All I know is that I completed my CFY under teletpractice per the 2022 guidelines and the cert director Amanda denied my CFY because I did not start seing kids until after winter break. I got both Direct and Indirect hours in December as well as a paycheck. We need another certification agency or they need to be held liable for their subjective chosing of who gets and does not get the CCC. That is the spirit of discrimination just because their cert director does not want to give you your CCC due to obvious subjective nitpicking based on what is required for the CCC. Nowhere does it say that I had to actually “see” my first kid in 2022. This causes an obvious inequality due to many positions now “requiring” the CCC. I cut ties with ASHA after that. Completely.
What are the CEU requirements for non-member CCCs?
Did you find the answer to this question as I’m 65 and retired but want to keep my state license and CCC’s that I worked hard for and small possibility that I may do some work in the field in the next 2 years. Although I’m retired and don’t have 25 consecutive time as a member (have 19yrs) ASHA still requires obtaining CEU’s until I have 25 yrs in. I’ll be 71 by then!
Hi, Michael. Thanks for the time you poured into fact checking and composing this article. In my opinion it’s a tautological argument, though, to say I should maintain my ASHA membership so my voice can be heard … when I have never once received even an acknowledgement from anyone at ASHA when I have reached out with questions or concerns. So, my opinion, it is an untestable position to say membership gives me a voice. In view of the 11% dues increase coming in 2025, I’m going to be dropping my ASHA membership this year. I appreciate you outlining the steps to do so, as I wouldn’t otherwise have known without doing the research myself.
Thank you again for the article, it was well written.
-Becky Mitchum, MS, CCC-SLP, CBIS